The German Nutrition Society (DGE) recommends 800 IU daily. 2,000 IU daily is the standard dose in many supplements. Some doctors work with 4,000 or even 10,000 IU daily for a confirmed deficiency. And recommendations circulate online that barely orient themselves around official guidelines anymore.
The confusion is understandable because genuinely different questions get mixed together: what is the minimum requirement to prevent a deficiency? What is the optimal supply for a healthy adult? And what is the maximum dose beyond which risks arise? This article separates these three questions.
What 800 IU means and why it is often not enough
The DGE recommends 800 IU (20 µg) daily as an estimate for adequate intake. This value is based on calculations targeting a certain 25-OH vitamin D level in the blood, specifically for people without meaningful vitamin D production of their own through sunlight.
The problem: 800 IU daily is a minimum value for a specific population group, not a universal recommendation for everyone. For people with a low starting level, higher body weight, darker skin, or limited absorption (certain conditions or medications), 800 IU is often not enough to build or maintain a sufficient level.
At the same time, 800 IU may be more than necessary for people with a good status and regular sun exposure in summer. The recommendation is an average value, not an individual prescription.
In practice: why 1,000 to 2,000 IU daily is the usual target range
In supplementation practice, 1,000 to 2,000 IU daily (25 to 50 µg) is by far the most common dosage range outside therapeutic applications. That is no coincidence.
In this range, the probability of building and maintaining a sufficient level is high for most adults. The risk of an overdose at these amounts over a longer time is minimal. At the same time, the difference from 800 IU is relevant: studies show that 800 IU daily is not enough for part of the population to reliably prevent deficiencies.
The European Food Safety Authority (EFSA) has set a tolerable upper level of 100 µg (4,000 IU) daily for adults. This value is the upper limit for ongoing consumption without increased risk, not the recommended daily dose.
Risk groups: who needs higher doses
Certain groups have increased needs and frequently do not reach a sufficient level with 800 IU:
People with a confirmed deficiency (25-OH vitamin D below 30 nmol/L) initially need higher doses to raise the level. Then lower maintenance doses.
Older people over 70 have a markedly reduced vitamin D synthesis in the skin and need a higher intake from supplements.
People with excess weight: since vitamin D is fat-soluble, part of it is stored in fat tissue and is not available for metabolism. The effectively available amount is lower at the same intake.
People with certain conditions that influence vitamin D absorption or activation, including kidney disease, chronic inflammatory bowel disease, or liver disease.
Daily dosing or a weekly depot: what works better
In practice, there are two approaches: low daily doses or higher weekly doses. Both lead to comparable average blood levels.
The BfR (the German Federal Institute for Risk Assessment), however, explicitly recommends avoiding very high single doses. Very high single servings (well above 4,000 IU at once, not as ongoing use) can lead to short-term peak levels that may be unfavorable. Low to medium doses at shorter intervals (daily or every two days) are the more stable model for ongoing supply.
Vitamin D dosage and vitamin K2: an important connection
The higher the vitamin D dose, the more relevant sufficient vitamin K2 becomes. Vitamin D increases calcium absorption in the gut. Vitamin K2 activates the proteins that direct this calcium into bones and keep it out of the vessels. With ongoing supplementation of 2,000 IU daily or more, a K2 supply of 100 to 200 µg daily as MK-7 is a sensible complement.
More on the interplay of D3 and K2 in the article Vitamin D3 and K2: why the combination achieves more than D3 alone.
RISE: the dosing logic explained
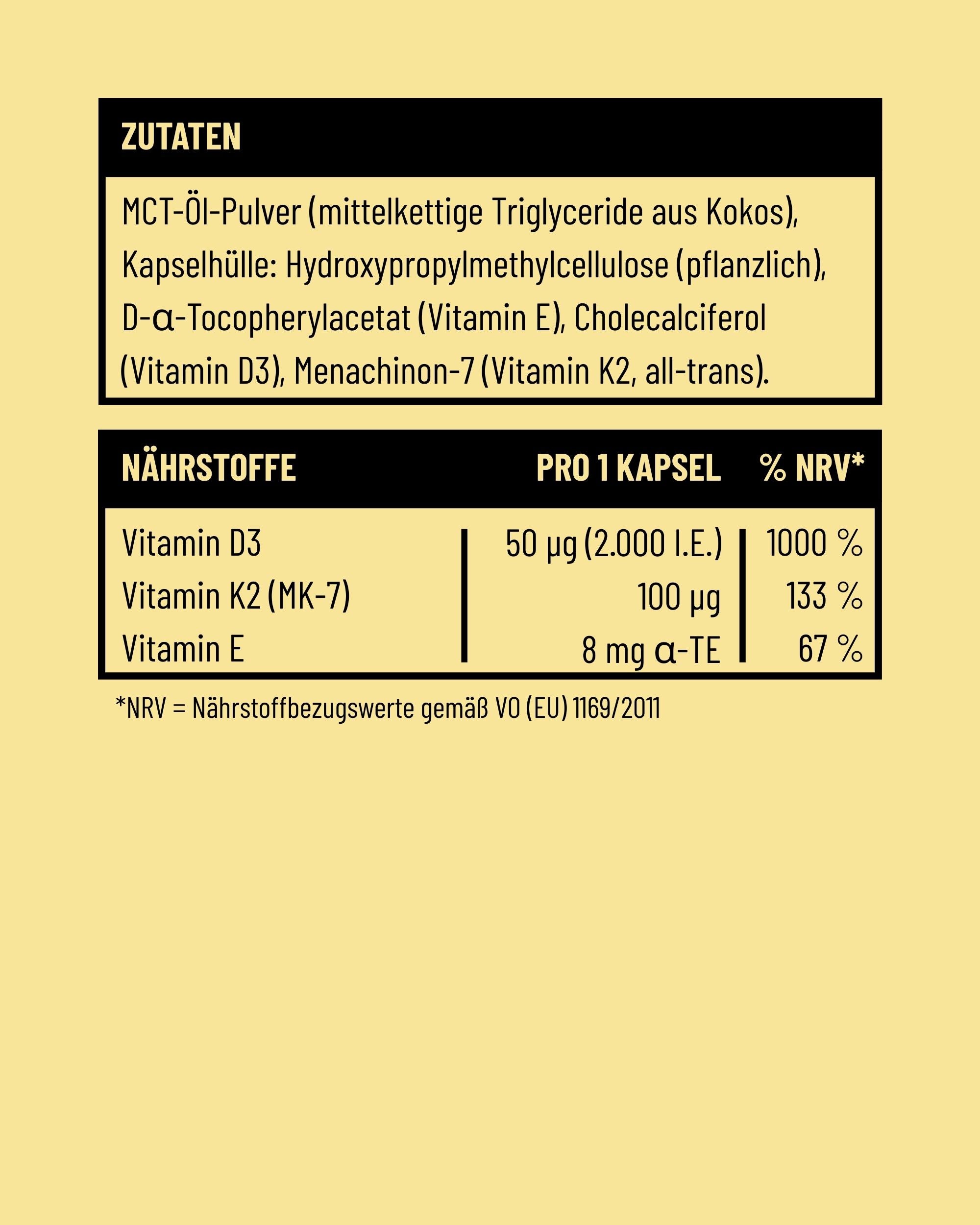
RISE by Fifty Five contains 50 µg of vitamin D3 (2,000 IU) per capsule, to be taken every two days. That results in an average daily dose of 25 µg (1,000 IU), which lies within the recommended target range.
The two-day dosing has a regulatory rationale: the BfR recommends a maximum daily dose of 20 µg for food supplements. RISE solves this with one capsule dose every two days that respects this framework while enabling a more effective supply than a plain 800 IU standard formulation. Added to this are 100 µg of K2 MK-7 per capsule, which fit exactly this dosing strategy. More on this in the complete RISE guide.
FAQ
Is 800 IU of vitamin D daily enough?
For part of the population with a good starting level and moderate sun exposure in summer, that can be enough. For people with a low starting level, older age, darker skin, or excess weight, it is often too little to build a sufficient level.
Is 2,000 IU daily too much?
For healthy adults, 2,000 IU (50 µg) lies well below the EFSA tolerable level of 4,000 IU daily. At this dosage, the risk of an overdose over a longer time is minimal. Still: anyone dosing higher permanently should have their level checked occasionally.
Does it make a difference whether I take it daily or every two days?
With the same total dose per period, the average blood levels are comparable. Small daily doses or a medium dose every two days lead to similar results. Very high single servings at long intervals (e.g. very high once weekly) are less advisable than more frequent moderate servings.
When should I discuss the dosage with a doctor?
When a blood test shows a deficiency, when long-term high doses (above 4,000 IU daily) are planned, when kidney disease, hypercalcemia, or certain other conditions exist, and when medications that interact with vitamin D are taken permanently.
Do I need more vitamin D in winter than in summer?
In winter, supplementation is generally more important since no production by the body takes place. The dosage does not necessarily have to be adjusted, though, if the goal is a year-round baseline supply. Anyone who regularly soaks up sun in summer can reduce supplementation in summer if desired.
Disclaimer:
This article is for informational purposes only and does not replace medical advice, diagnosis, or treatment by a physician or pharmacist. The information provided here should not be used for self-diagnosis or self-treatment. Food supplements are no substitute for a balanced, varied diet and a healthy lifestyle. For any health questions or complaints, please always consult a doctor you trust. Fifty Five accepts no liability for any inconvenience or harm resulting from the use of the information presented here.
Sources
- EFSA. Dietary reference values for vitamin D. EFSA Journal 2016;14(10):4547.
- EFSA. Scientific Opinion on the Tolerable Upper Intake Level of vitamin D. EFSA Journal 2012;10(7):2813.
- EFSA. Dietary reference values for vitamin K. EFSA Journal 2017;15(5):4780.
- German Nutrition Society (DGE). D-A-CH reference values – vitamin D.
- Robert Koch Institute (RKI). DEGS – German Health Interview and Examination Survey for Adults (vitamin D status).










Multivitamin Side Effects: What Really Happens When You Take Too Much
Fish Oil or Algae Oil: Where Omega-3 Really Comes From
Share: