
Vitamin D3 increases calcium absorption. That is well known. What is less known: more calcium in the blood alone is not the goal, it is an intermediate step. Where this calcium ends up is the actually relevant question. This is exactly where vitamin K2 comes in.
The combination of D3 and K2 has been researched more intensively for some years. The basic connection is well established biologically: the two vitamins complement each other in the body's calcium regulation in a way that neither substance alone can achieve.
How vitamin D3 influences calcium absorption
Vitamin D3 (cholecalciferol) is converted in the liver to 25-OH vitamin D3 and then in the kidney to the active form 1,25-OH vitamin D3 (calcitriol). Calcitriol is a hormone that stimulates the production of transport proteins in the small intestine. These proteins take up calcium from food and channel it into the blood.
The result: with sufficient vitamin D supply, the body absorbs considerably more calcium from a calcium-rich meal than in a deficiency. Vitamin D contributes to normal absorption and utilization of calcium and contributes to the maintenance of normal bones.
That is physiologically sensible. The skeleton, the muscles, and the nervous system need calcium. Having more calcium in the blood is the first step. The second step is that this calcium ends up where it is needed.
What vitamin K2 has to do with it
Vitamin K2 is a group of fat-soluble vitamins (menaquinones) involved in the activation of certain proteins. Two of them are decisive for calcium regulation.
Osteocalcin is a protein found in bones and teeth. It binds calcium and anchors it in the bone matrix. Without sufficient K2, osteocalcin remains inactive (undercarboxylated) and cannot fulfill this task. With sufficient K2, it is activated and contributes to the incorporation of calcium into the bone structure.
Matrix Gla protein (MGP) is the most effective known inhibitory protein against vascular calcification. It prevents calcium from depositing in the walls of blood vessels and other soft tissues. MGP is also dependent on vitamin K2 to be activated.
Vitamin K2 contributes to the maintenance of normal bones and contributes to normal blood clotting.
The interplay: D3 increases the need for K2
Anyone who absorbs more calcium into the blood (through vitamin D) also needs more capacity to direct this calcium. That means: more K2 to sufficiently activate osteocalcin and MGP.
At low D3 doses (800 IU daily), this effect is limited. At higher doses (2,000 IU daily or more), sufficient K2 supply becomes more relevant. Anyone permanently supplementing high-dose D3 without paying attention to K2 may be supplementing only halfway.
The research is not yet conclusive. Long-term studies specifically examining the combination of D3 and K2 on hard clinical endpoints (bone density, fracture rate, cardiovascular health) are ongoing or still outstanding. But the biological mechanisms are well documented.
Which K2 form is the right one
Not all vitamin K2 forms are the same. The forms relevant for supplementation are MK-4 and MK-7.
MK-4 has a very short half-life of about one hour in the blood. For continuous biological activity, very frequent intake would be necessary. In studies, MK-4 was mostly used in very high dosages (15 mg daily) that are not practically relevant for typical supplementation.
MK-7 has a half-life of about 72 hours. That means: a single daily or every-other-day dose stays active in the body considerably longer. For everyday supplementation, MK-7 is the obvious choice.
Within MK-7, the all-trans configuration is the biologically active form. Cis isomers have no proven efficacy. When selecting a product, all-trans MK-7 should be on the label or documented by the raw material certification.
RISE: D3 and K2 in coordinated dosing
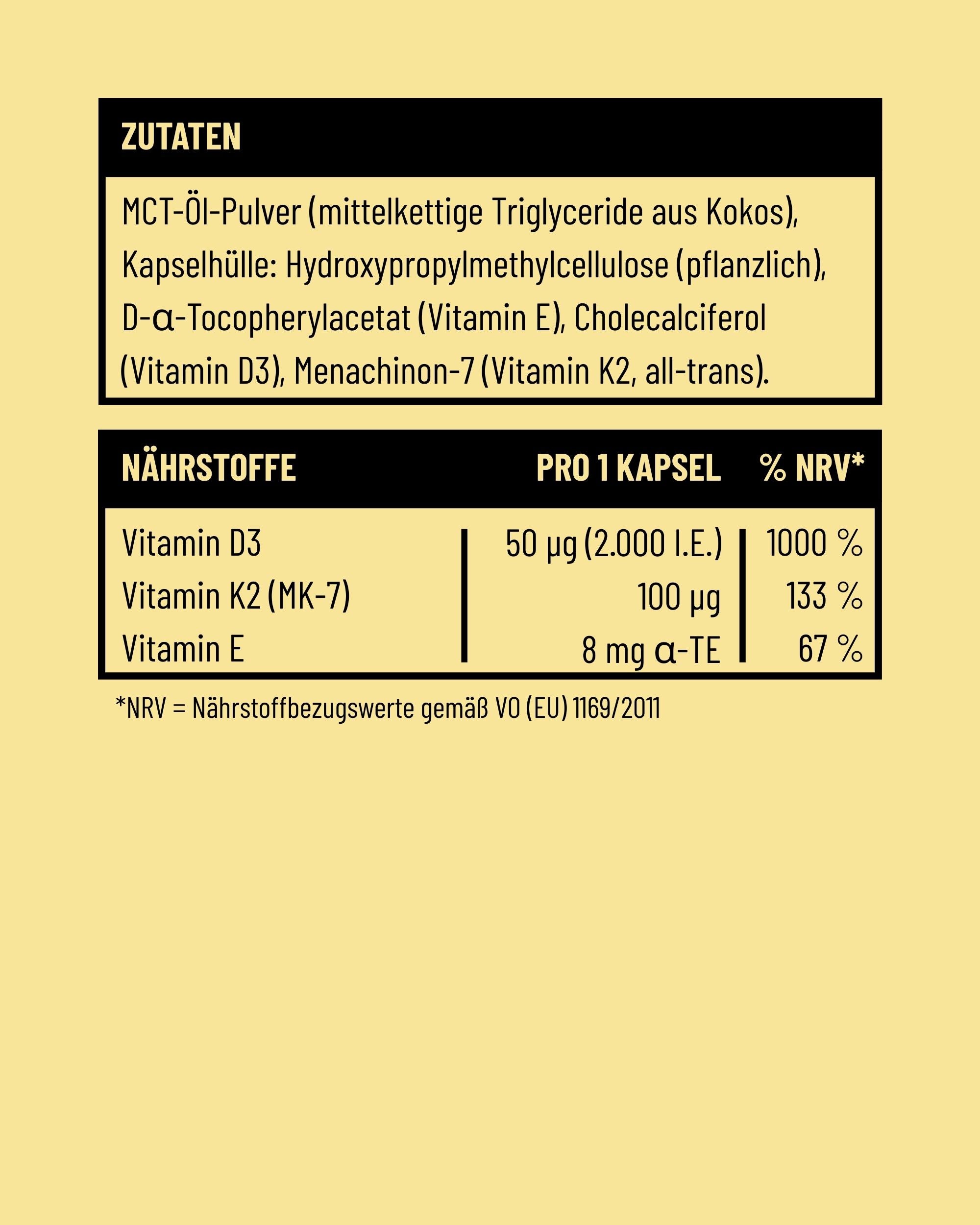
RISE by Fifty Five combines 50 µg of vitamin D3 with 100 µg of vitamin K2 as MK-7 all-trans in a micro capsule, to be taken every two days. The dosing is coordinated: 1,000 IU of vitamin D3 (as a daily average) and 50 µg of K2 MK-7 daily (as a daily average) both lie in a range that enables a biologically relevant supply without going into risky territory. More on the system logic in the complete RISE guide.
FAQ
Do I have to take K2 if I supplement D3?
At low D3 doses (800 IU), it is not an urgent necessity. With ongoing intake of 2,000 IU and more, sufficient K2 is a smart complement to support calcium distribution in the body.
How much K2 do I need for a certain D3 dose?
There is no officially set ratio. In practice, at 1,000 to 2,000 IU of D3 daily, 100 to 200 µg of K2 MK-7 daily is typically recommended. This range lies well above the official intake recommendation for vitamin K but is well tolerated with MK-7.
Can too much K2 cause problems?
Vitamin K2 MK-7, unlike synthetic vitamin K, is well tolerated, even at higher amounts. A relevant contraindication exists when taking vitamin K antagonists (certain blood thinners like warfarin). Anyone taking such medications should discuss K2 supplementation with a doctor.
Is K2 also recommendable for children?
Vitamin K2 is a natural component of the diet, especially in fermented foods. For children, targeted supplementation is less established than for adults. With a specific reason (e.g. higher-dose vitamin D supplementation), consultation with the pediatrician is sensible.
What is the difference between vitamin K1 and K2?
K1 occurs mainly in green vegetables and is utilized predominantly in the liver for blood clotting. K2 (especially MK-7) is better transported into bones, vessels, and other tissues, where it takes on the calcium-regulating function. For bone health and vascular protection, K2 is the relevant form.
Disclaimer:
This article is for informational purposes only and does not replace medical advice, diagnosis, or treatment by a physician or pharmacist. The information provided here should not be used for self-diagnosis or self-treatment. Food supplements are no substitute for a balanced, varied diet and a healthy lifestyle. For any health questions or complaints, please always consult a doctor you trust. Fifty Five accepts no liability for any inconvenience or harm resulting from the use of the information presented here.










Single Vitamin or Multivitamin: When a Combination Product Is Smarter, and When It Is Not
Omega-3 Dosage: How Much DHA and EPA You Need Daily
Share: